
Zika NS3 helicase:RNA complex
New high resolution structure of ZIKV NS3 helicase is available in Protein Data Bank (PDB ID: 5MFX)


New high resolution structure of ZIKV NS3 helicase is available in Protein Data Bank (PDB ID: 5MFX)

Infection of pregnant women by Asian lineage strains of Zika virus (ZIKV) has been linked to brain abnormalities in their infants, yet it is uncertain when during pregnancy the human conceptus is most vulnerable to the virus. We have examined two models to study susceptibility of human placental trophoblast to ZIKV: cytotrophoblast and syncytiotrophoblast derived from placental villi at term and colonies of trophoblast differentiated from embryonic stem cells (ESC). The latter appear to be analogous to the primitive placenta formed during implantation. The cells from term placentas, which resist infection, do not express genes encoding most attachment factors implicated in ZIKV entry but do express many genes associated with antiviral defense. By contrast, the ESC-derived trophoblasts possess a wide range of attachment factors for ZIKV entry and lack components of a robust antiviral response system. These cells, particularly areas of syncytiotrophoblast within the colonies, quickly become infected, produce infectious virus and undergo lysis within 48 h after exposure to low titers (multiplicity of infection > 0.07) of an African lineage strain (MR766 Uganda: ZIKVU) considered to be benign with regards to effects on fetal development. Unexpectedly, lytic effects required significantly higher titers of the presumed more virulent FSS13025 Cambodia (ZIKVC). Our data suggest that the developing fetus might be most vulnerable to ZIKV early in the first trimester before a protective zone of mature villous trophoblast has been established. Additionally, MR766 is highly trophic toward primitive trophoblast, which may put the early conceptus of an infected mother at high risk for destruction.

The Zika virus (ZIKV) causes various neurologic defects including microcephaly and the Guillain-Barré syndrome. However, little is known about how ZIKV causes those diseases or which viral protein(s) is responsible for the observed cytopathic effects involved in restricted neuronal cellular growth, dysregulation of the cell cycle, and induction of cell hypertrophy or cell death. A genome-wide analysis of ZIKV proteins and peptides was conducted using fission yeast as a surrogate host. Seven ZIKV proteins conferred various cytopathic effects in which NS4A-induced cellular hypertrophy and growth restriction were mediated through the target of rapamycin (TOR) cellular stress-response pathway. These findings provide a foundation for identifying viral pathogenicity factors associated with the ZIKV diseases.

Until it burst onto the scene earlier this year, Zika was an obscure, little-known virus. As a result, scientists know little about how it works. Over the past year, they have learned that it can cause a range of dangerous health problems, including birth defects such as microcephaly and neurological problems such as Guillain-Barré syndrome. But they don’t know which Zika protein or proteins are causing harm, or exactly how these proteins cause damage.
Now, a new study by scientists at the University of Maryland School of Medicine (UM SOM) has for the first time identified seven key proteins in the virus that may be the culprits behind this damage. The study is the first comprehensive description of the Zika virus genome. The study was published today in the journal Proceedings of the National Academy of Sciences.


The current Zika virus (ZIKV) epidemic is characterized by severe pathogenicity in both children and adults. Sequence changes in ZIKV since its first isolation are apparent when pre-epidemic strains are compared with those causing the current epidemic. However, the residues that are responsible for ZIKV pathogenicity are largely unknown. Here we report the cryo-electron microscopy (cryo-EM) structure of the immature ZIKV at 9-Å resolution. The cryo-EM map was fitted with the crystal structures of the precursor membrane and envelope glycoproteins and was shown to be similar to the structures of other known immature flaviviruses. However, the immature ZIKV contains a partially ordered capsid protein shell that is less prominent in other immature flaviviruses. Furthermore, six amino acids near the interface between pr domains at the top of the spikes were found to be different between the pre-epidemic and epidemic ZIKV, possibly influencing the composition and structure of the resulting viruses.

The Public Health Emergency of International Concern (PHEIC) declared by the Director-General of WHO has led the world to an urgent and coordinated response, providing the understanding that Zika virus infection and associated consequences represent a highly significant long-term problem that must be managed by WHO, States Parties and other partners in a way that other infectious disease threats are managed.
The EC originally recommended a PHEIC in February 2016 on the basis of an extraordinary cluster of microcephaly and other neurological disorders reported in Brazil, following a similar cluster in French Polynesia and geographic and temporal association with Zika virus infection which required urgent and coordinated and research. Because research has now demonstrated the link between Zika virus infection and microcephaly, the EC felt that a robust longer-term technical mechanism was now required to manage the global response.
As a result, the EC felt that Zika virus and associated consequences remain a significant enduring public health challenge requiring intense action but no longer represent a PHEIC as defined under the IHR. Many aspects of this disease and associated consequences still remain to be understood, but this can best be done through sustained research. The EC recommended that this should be escalated into a sustained programme of work with dedicated resources to address the long-term nature of the disease and its associated consequences.
The Committee reviewed the recommendations made at its previous meetings and agreed that WHO and partners had systematically addressed their advice. Furthermore, the EC reviewed and agreed to the WHO Zika transition plan outlined to establish the longer-term response mechanism which delivers the strategic objectives already identified in the Zika Strategic Response Plan.
Based on this advice, the Director-General declared the end of the Public Health Emergency of International Concern (PHEIC). The Director-General reissued the Temporary Recommendations from the previous meetings of the Committee which will be incorporated into the longer-term response mechanism. The Director-General thanked the Committee Members and Advisors for their advice over the past year.

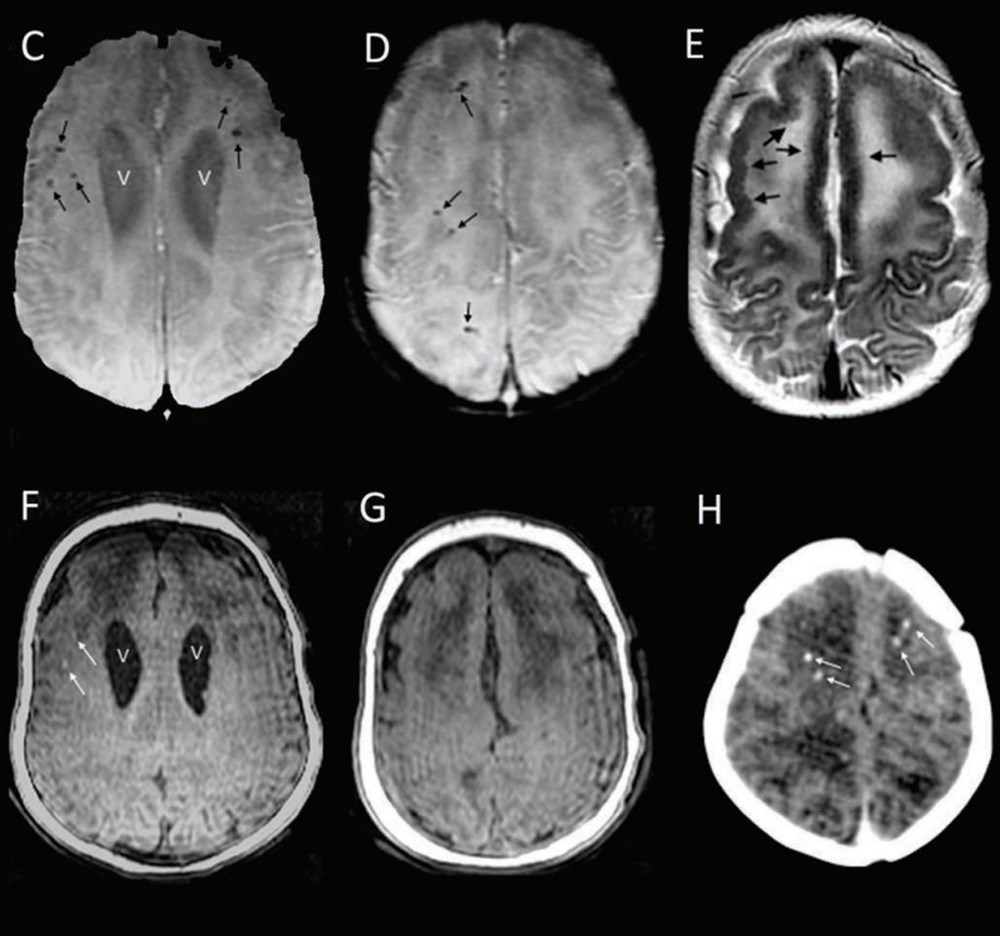
Congenital Zika virus infection can cause microcephaly and severe brain abnormalities. Congenital Zika syndrome comprises a spectrum of clinical features; however, as is the case with most newly recognized teratogens, the earliest documented clinical presentation is expected to be the most severe. Initial descriptions of the effects of in utero Zika virus infection centered prominently on the finding of congenital microcephaly. To assess the possibility of clinical presentations that do not include congenital microcephaly, a retrospective assessment of 13 infants from the Brazilian states of Pernambuco and Ceará with normal head size at birth and laboratory evidence of congenital Zika virus infection was conducted. All infants had brain abnormalities on neuroimaging consistent with congenital Zika syndrome, including decreased brain volume, ventriculomegaly, subcortical calcifications, and cortical malformations. The earliest evaluation occurred on the second day of life. Among all infants, head growth was documented to have decelerated as early as 5 months of age, and 11 infants had microcephaly. These findings provide evidence that among infants with prenatal exposure to Zika virus, the absence of microcephaly at birth does not exclude congenital Zika virus infection or the presence of Zika-related brain and other abnormalities. These findings support the recommendation for comprehensive medical and developmental follow-up of infants exposed to Zika virus prenatally. Early neuroimaging might identify brain abnormalities related to congenital Zika infection even among infants with a normal head circumference.

Zika virus (ZIKV) infection of pregnant women can cause congenital malformations including microcephaly, which has focused global attention on this emerging pathogen. In addition to transmission by mosquitoes, ZIKV can be detected in the seminal fluid of affected males for extended periods of time and transmitted sexually. Here, using a mouse-adapted African ZIKV strain (Dakar 41519), we evaluated the consequences of infection in the male reproductive tract of mice. We observed persistence of ZIKV, but not the closely related Dengue virus (DENV), in the testis and epididymis of male mice, and this was associated with tissue injury that caused diminished testosterone and inhibin B levels, and oligospermia. ZIKV preferentially infected spermatogonia, primary spermatocytes, and Sertoli cells in the testis, resulting in cell death and destruction of the seminiferous tubules. Less damage was observed with a contemporary Asian ZIKV strain (H/PF/2013), in part because this virus replicates less efficiently in mice. The extent to which these observations in mice translate to humans remains unclear, but longitudinal studies of sperm function and viability in ZIKV-infected humans seem warranted.
In this Correspondence, we show that Zika virus RNA might be present in the female genital tract up to day 11 after symptoms onset, but with a genital clearance observed at day 17 before urine clearance. Zika virus clearance from the female genital tract needs to be assessed by large and longitudinal studies with infectiousness evaluation. These data should be used to change recommendations for prevention of sexual transmission of Zika virus.

Recent outbreaks of Zika virus in Oceania and Latin America, accompanied by unexpected clinical complications, made this infection a global public health concern. This virus has tropism to neural tissue, leading to microcephaly in newborns in a significant proportion of infected mothers. The clinical relevance of this infection, the difficulty to perform accurate diagnosis and the small amount of data in literature indicate the necessity of studies on Zika infection in order to characterize new biomarkers of this infection and to establish new targets for viral control in vertebrates and invertebrate vectors. Thus, this study aims at establishing a lipidomics profile of infected mosquito cells compared to a control group to define potential targets for viral control in mosquitoes. Thirteen lipids were elected as specific markers for Zika virus infection (Brazilian strain), which were identified as putatively linked to the intracellular mechanism of viral replication and/or cell recognition. Our findings bring biochemical information that may translate into useful targets for breaking the transmission cycle.









")